Current Case: Spring 2024
Contributed by: Mustafa Donmez, MD and Pegah Afra, MD, UMass Chan Medical School, Worcester, MA, USA
Case Presentation
41-year-old right-handed woman with drug-resistant focal epilepsy (right temporal) manifest as focal impaired awareness seizures (FIAS) with and without bilateral tonic -clonic activity presents to the ED with worsening seizure frequency. She is s/p RNS 320 implantation, which resulted in a marked decrease in FIAS frequency and severity. In the ER, the patient has a CT scan, showing neurostimulator location over the right parietal bone and two RNS leads (strip over the right temporal neocortex; depth in the right mesial temporal area). The patient was admitted emergently to the epilepsy monitoring unit (EMU) and scalp vEEG recordings were performed using standard 10-20 system electrodes. In the past her EEGs have repeatedly shown right temporal interictal epileptiform discharges (RT-IED). vEEG showed intermittent bursts as depicted in figure 1 and 2 below
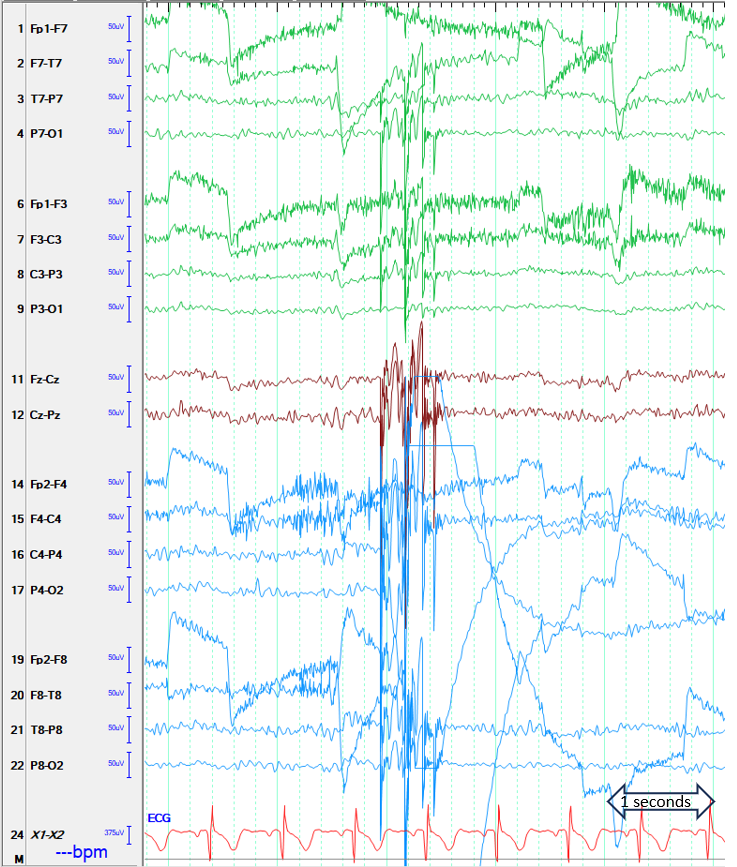
Figure 1. Illustration of one of the intermittent bursts (LFF 1 Hz, HFF 70 Hz, Sensitivity 7 uV/mm)
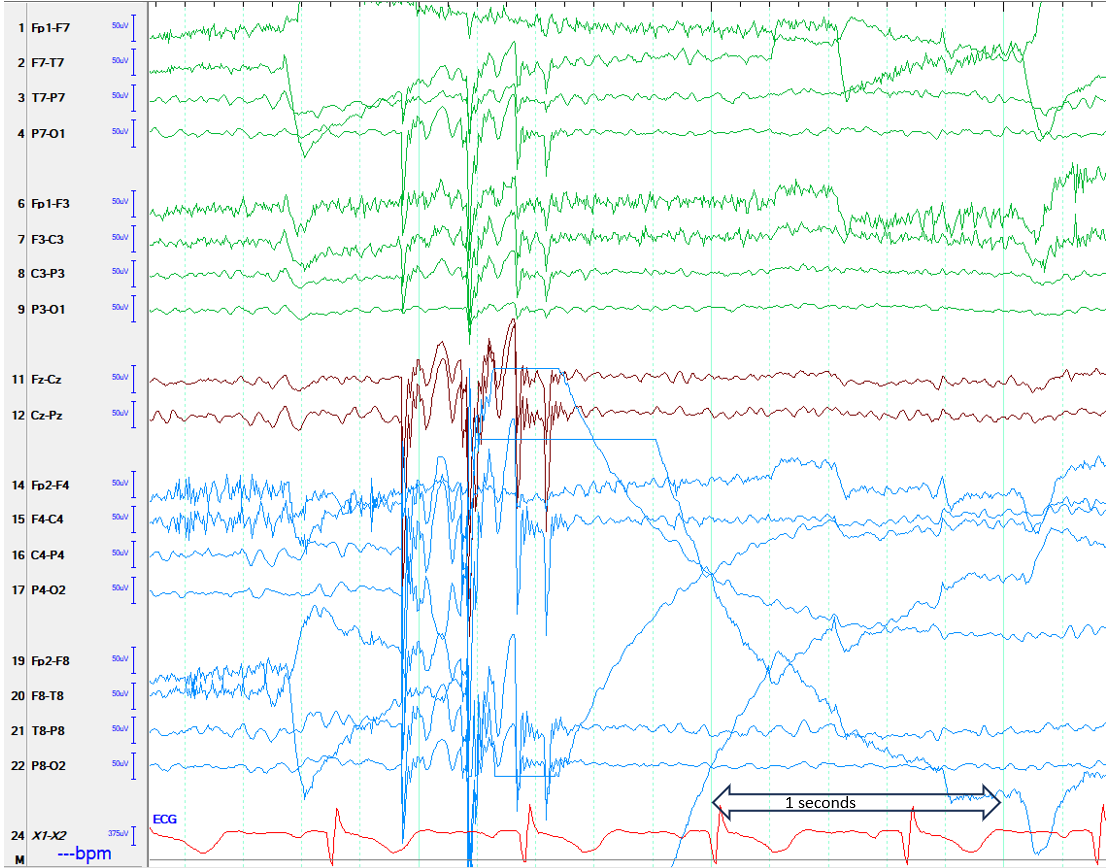
Figure 2. Illustration of the intermittent bursts at lower time display (LFF 1 Hz, HFF 70 Hz, Sensitivity 7 uV/mm)
Question 1: In the figure, what is the arrow pointing to?
- Generalized spike and slow wave (GSSW) complexes
- Physiological artifact: GSSW-like activity induced by glossokinetic movements
- Non-physiological artifact: GSSW-like activity induced by RNS
- Non-physiological artifact: GSSW-like activity secondary to lose ground causing motion sensitivity
Answer: (click here)
Correct answer: C. Non-physiological artifact: GSSW-like activity induced by RNS
The arrow points to intermittent activity similar to generalized bursts of spike and slow wave discharges (GSSW-like) that was asymmetric with maxima in the right parietal region. The GSSW-like burst is somewhat irregular with burst duration of approximately 600 msec, and the contained spike-like frequency was about 6-10 Hz.. The unusual morphology and non-physiologic localization suggests artifact1-3. This activity does not resemble epileptic discharges, glossokinetic artifact; lose ground typically causes motion sensitivity(1).
Question 2: How do you prove that you are correct
- Turn the RNS off; focal leads in the right temporal neocortex and mesial temporal area will not help this patient’s epilepsy
- Ask the patient to say lalala, tatata (where tip of the tongue touches the palate) to reproduce the glossokinetic artifact
- Interrogate RNS and start manual stimulation via programmer to see if the artifact is reproducible
- Ask the technologist to re-gel or change the ground electrode
Answer: (click here)
Correct answer: C. Interrogate RNS and start manual stimulation via programmer to see if the artifact is reproducible.
The only way to prove is to reproduce the artifact by manual stimulation of RNS via the programmer. This was performed and temporal correlation to manual stimulation was established (i.e. a similar artifact appeared with each manual stimulation of RNS at bed side). It is unclear whether the RNS-induced EEG-artifact characteristics are due to the location of the implanted RNS generator in the skull or the location of signal delivery (i.e. implanted lead location). This case adds to the armamentarium of non-physiological device-related artifacts2-3, emphasizing the importance of familiarity with the unique EEG characteristics of device-related artifacts and the need to distinguish them from epileptiform activity(1).
References:
- Tatum WO, Dworetzky, Schomer DL (2011). Artifact and Recording Concepts in EEG. J Clin Neurophysiol. 28: 252-263.
- Nascimento FA, Chu J, Fussner S, Krishnan V, Maheshwari A, Gavvala JR (2021). Neurostimulation EEG artifacts: VNS, RNS and DBS. Arq Neuropsiquiatr. 79 (752-753)
- Arafat T, Miron G, Strauss I, Fahoum F (2022). Electrodiagnostic artifacts due to neurostimulation for drug resistant epilepsy. Epilepsy Behav Rep. 20:100566
