Featured Case - October 2017
Featured Case
Contributed by: Jennifer M. Martinez-Thompson, MD and Ruple S. Laughlin, MD
Mayo Clinic Rochester
Clinical Presentation:
A 71 year-old man presented for evaluation of head drop, dysphagia, and proximal limb weakness. He had been diagnosed with seronegative autoimmune myasthenia gravis locally with partial response to pyridostigmine. He had lid ptosis and mild facial weakness without ophthalmoparesis, neck flexor and extensor weakness, asymmetric scapular winging, and moderate limb-girdle pattern weakness without reflex or sensory abnormalities on his neurologic examination. There was no clinical myotonia.
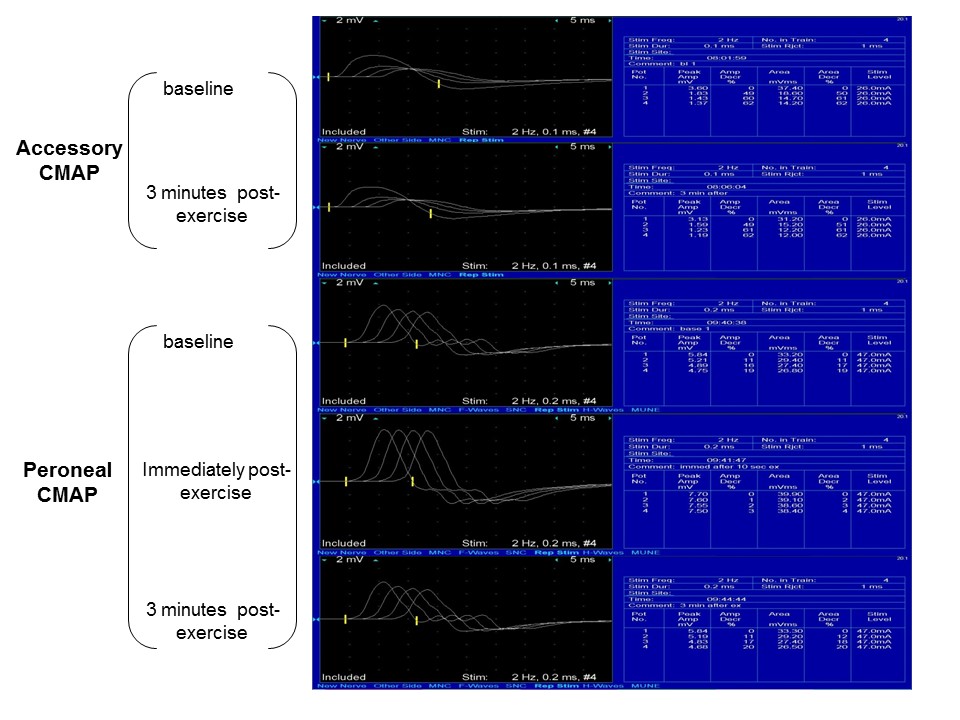
Standard nerve conduction studies were normal. Two-hertz (Hz) repetitive stimulation of the ulnar and facial nerves showed no decrement at baseline and after one minute of exercise. Baseline and post-exertion repetitive stimulation of the accessory and peroneal nerves is shown in the figure below. The immediate post-exercise accessory compound muscle action potential (CMAP) is not shown as there was no repair. Needle EMG showed short-duration, low amplitude, polyphasic motor unit potentials with rapid recruitment diffusely with rare fibrillation potentials. Varying motor unit potentials were noted in the deltoid and tibialis anterior muscles.

Question 1: Can decrement be a finding in a primary myopathic process?
- Yes
- No
Answer: (click here)
A1: Correct answer is a (yes).
Choice 1. There can be decrement on repetitive stimulation in primary myopathic or neurogenic disorders, although typically the decrement is less prominent than what is seen in neuromuscular junction disease. Up to 20% decrement has been reported on repetitive stimulation at baseline in myopathy, although some myopathies with associated neuromuscular transmission failure due to alteration in end-plate physiology can result in higher decrement values as seen in this case.
Rodriguez Cruz PM. Congenital myopathies with secondary neuromuscular transmission defects; a case report and review of the literature. Neuromuscul Disord 2014; 24: 1103-10.
Question 2: Which myopathy(ies) have been associated with a defect of neuromuscular transmission?
- Myotonic dystrophy type 1 and 2
- Inclusion body myositis
- Steroid-associated myopathy
- Centronuclear myopathy
- Dermatomyositis
Answer: (click here)
A2: Correct answer is d (Centronuclear myopathy).
Choice 4. The centronuclear myopathies are a histopathologically defined, heterogeneous group of myopathies that have been associated with post-synaptic neuromuscular transmission defects. Pathologic findings consist of prominent, centrally located nuclei in > 70% of muscle fibers. This patient had evidence of a myopathy on his triceps muscle biopsy with most fibers harboring central nuclei. Mutations most commonly associated with centronuclear pathology include MTM1 (myotubularin), DNM2 (dynamin-2), BIN-1 (amphyiphysin-2), and RYR-1 (ryanodine receptor), each with a variable age of symptom onset and severity, fatigability, significant decrement on repetitive nerve stimulation, and partial response to pyridostigmine and/or 3,4-diaminopyridine. Electron microscopy evaluation of muscle biopsies in affected individuals with these mutations have shown muscle end-plate and junctional fold abnormalities, which are postulated to variably affect neuromuscular transmission.
Robb et al. Impaired neuromuscular transmission and response to acetylcholinesterase inhibitors in centronuclear myopathies. Neuromuscul Disord 2011; 21 (6): 379-86.
Liewluck et al. Endplate structure and parameters of neuromuscular transmission in sporadic centronuclear myopathy associated with myasthenia. Neuromuscul Disord 2011; 21(6): 387-95.