Featured Case -July 2017
Featured Case
Contributed by Orhan Bican, MD and Lauren Lahdan Heidarian, MD
University of Utah
Clinical Presentation:
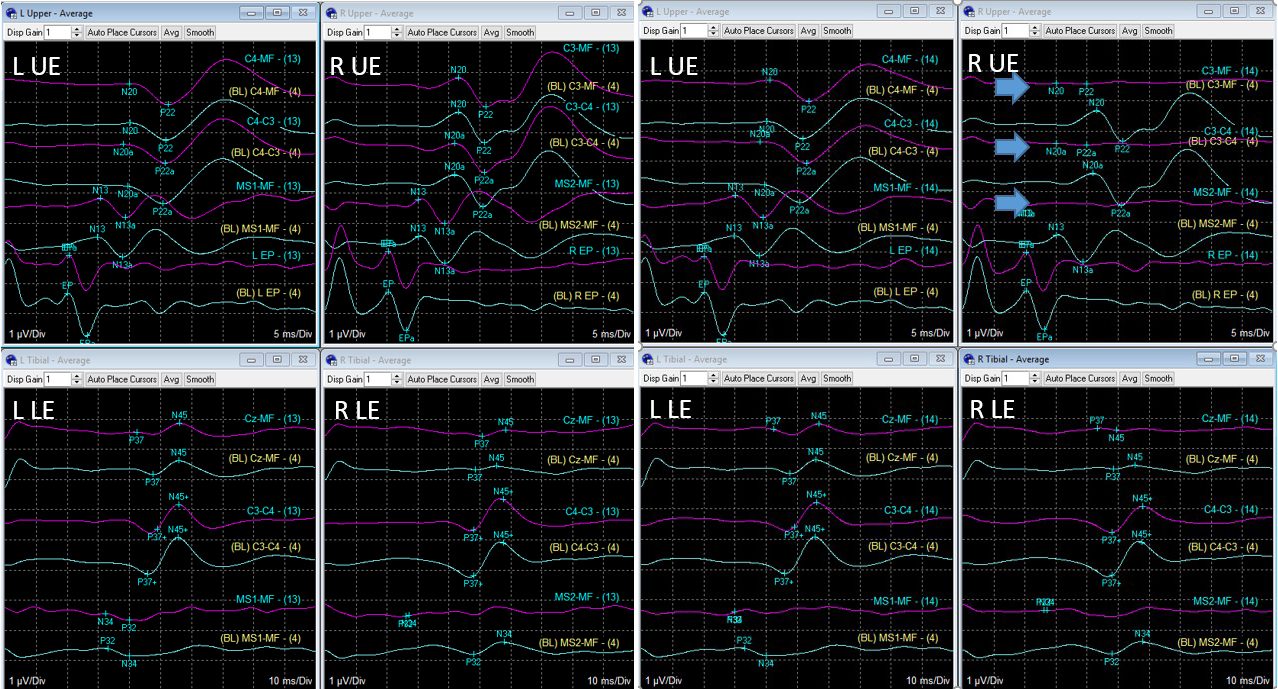
The patient is a 61-year-old undergoing posterior cervical fusion C4-6 and laminectomy C4-7. Somatosensory evoked potentials (SSEP) after bilateral median and posterior tibial nerve stimulation was performed. During laminectomy, there was loss of sensory response from right upper extremity. Blue traces indicate baseline recordings and Purple traces are active recordings. (L: Left, R: right, UE: upper extremity, LE: lower extremity):
Question 1: What is the most likely etiology to account for this neurophysiologic change?
- Anesthesia
- Neuromuscular blocking agent
- Hypothermia
- Loss of peripheral stimulation
- Impairment of impulse conduction proximal to Erb potential
Answer: (click here)
A1: Correct answer is e.
Neurophysiologic changes due to anesthesia can occur when volatile anesthetics are used, and can also be occasionally encountered with propofol accumulation in prolonged surgeries when high dose total intravenous anesthesia is utilized. Neurophysiologic changes due to anesthesia predominantly compromise cortical responses. Subcortical potentials and peripheral potentials are usually spared or affected to a lesser degree. Neurophysiologic changes due to anesthesia are also expected to be global, involving responses from more than one extremity. In this case, a focal change was seen in cortical and subcortical responses from the right upper extremity only.
Administration of neuromuscular blocking agents usually result in disappearance of the muscle artifact, that can interfere with averaging of somatosensory evoked potential responses. Thereby the net effect of administration of neuromuscular blocking agent would be enhancement somatosensory evoked potential amplitudes.
Hypothermia is the most common cause for prolongation of central waveforms latencies intraoperatively. Deep hypothermia can be utilized in vascular procedures and can result in prolongation of latencies prior to complete disappearance of SSEP responses. Similar to anesthesia induced SSEP changes, hypothermia related changes would be expected to result in global changes in all extremities.
Loss of peripheral stimulation can be ruled out in this case due to preservation of Erb potential. Peripheral potentials (Erb, Popliteal) are extremely useful as control potentials and can rule out loss of peripheral stimulation which is a common technical problem due to displacement of the stimulating electrode.
Preservation of the Erb potential indicates the stimulation is being delivered and can be recorded from brachial plexus. In this case, the change was related to a conduction block proximal to Erb potential.
Question 2: Where would you best localize the lesion in the light of these findings?
- Dorsal column proximal to C6 vertebrate level
- Dorsal column distal to C6 vertebrate level
- C6 nerve root
- C7 nerve root
- Involvement of multiple nerve roots between C6-T1
Answer: (click here)
A2: Correct answer is e.
Somatosensory evoked potentials overall are more sensitive in detecting spinal cord injuries than root injuries as median or ulnar nerve stimulation travels through multiple nerve roots and involvement of a single nerve root usually does not result in critical amplitude decrease. However, in the presence of a spinal cord injury, one would also expect involvement of the ipsilateral sensory responses from the lower extremity. In this case, preservation of the bilateral lower extremity sensory responses argues against a significant spinal cord injury. These findings could be best explained by involvement of multiple nerve roots between right C6-T1 levels. In this case, there was a simultaneous change (not included in the figure) of the motor evoked potential (MEP) responses from the right extensor digitorum communis and abductor pollicis brevis muscles, with preservation of MEP responses from the right trapezius, deltoid and abductor hallucis muscles. The MEP findings also suggest involvement of multiple nerve roots between C6-T1 levels.