Featured Case - December 2017
Featured Case
Contributed by: Sotiris Mitropanopoulos, MD & Lily Wong-Kisiel, MD
Mayo Clinic College of Medicine, Rochester, MN
Clinical Presentation: Video EEG monitoring in a 9 year old suspected of ESES
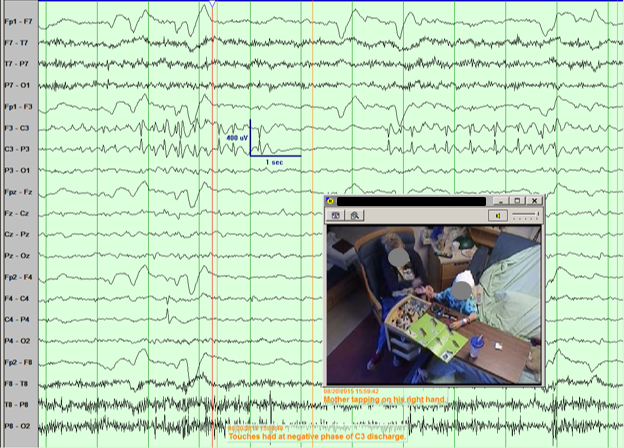
A 9 year-old right-handed male with neurofibromatosis type 1, attention deficit hyperactivity disorder, intellectual disability with academic plateau, and electrical status epilepticus during sleep (ESES) was admitted to overnight video EEG monitoring for ESES evaluation. He has never had a clinical seizure. The EEG showed seemingly spontaneous focal spike-and-wave discharges coming from both the right and left central regions during wakefulness. These discharges often occurred while the child was playing with the touchscreen tablet or when his palm was tapped repeatedly during play (Figures 1-3). During sleep there was marked activation of independent left and right central discharges typical of ESES.
Figure 1 - Tapping touchscreen with right thumb. EEG: Bipolar montage with a time base 30 mm/sec, sensitivity 20 µV/mm, high frequency filter at 70 Hz, low frequency filter at 1 Hz.
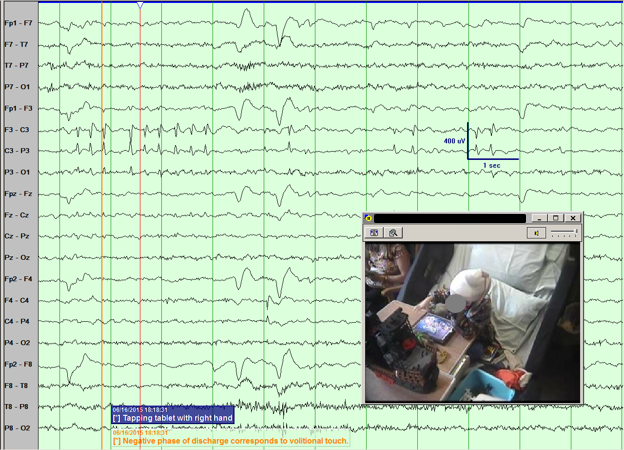
Figure 2 - Tapping touchscreen with left index finger. EEG: Bipolar montage with a time base 30 mm/sec, sensitivity 20 µV/mm, high frequency filter at 70 Hz, low frequency filter at 1 Hz.
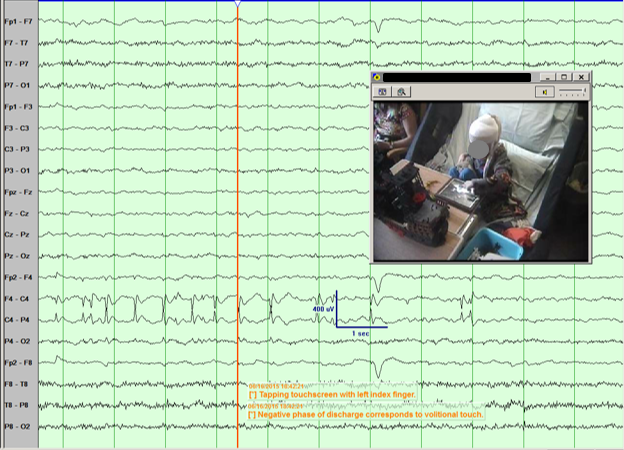
Figure 3 - Rhythmic tapping on the right palm. EEG: Bipolar montage with a time base 30 mm/sec, sensitivity 20 µV/mm, high frequency filter at 70 Hz, low frequency filter at 1 Hz.
Question 1: What do these discharges represent?
- Interictal activity of childhood epilepsy with centrotemporal spikes.
- Tactile-evoked discharges.
- Electrode artifact.
- Interictal activity of atypical childhood epilepsy with centrotemporal spikes.
Answer & Discussion: (click here)
A1: Correct answer is: Tactile-evoked discharges(TED)
Choice B. These figures demonstrate tactile-evoked discharges (TED). The first large scale study investigating this phenomenon was conducted in 1981 by de Marco and Tassinari. In 15,000 children referred for EEG, 155 children were found to have TED. Of these 155 patients, 16 developed epilepsy. Among those who developed epilepsy, an electroclinical progression consisting of spontaneous discharges in the same topographic distribution during sleep, then during wakefulness and sleep, and finally spontaneous seizures (1). In another study in 1999 by de Marco and Calzolari, 566 children with TED were evaluated by assessing the relationship between TED, spontaneous discharges, and somatosensory evoked potentials. The authors concluded that TED were associated with increased risk of epilepsy (2). The latest retrospective study of TED was conducted by Langill and Wong in 2003. This study included 304 patients with rolandic discharges that were either spontaneous (NT), spontaneous and enhanced with tactile stimulation (TE), or tactile (tapping) only (TO) discharges (3). Although the overall incidences of seizures in the NT, TE, and TO cohorts were 70.7%, 54.3%, and 48.6%, respectively, when looking at patients who had normal EEG background and no other epileptiform abnormalities, the incidence of seizures were low among the tactile-enhanced (26%) and tactile-only (35%) cohorts, suggesting that TED may not be a reliable marker for future development of epilepsy (3). In addition, there was a higher incidence of abnormal intelligence in NT and TE groups vs the TO group. No patient had the same electroclinical progression described by de Marco and Tassinari (1). Our patient would likely be grouped in the TE group from the Langill and Wong study, since these discharges would occur spontaneously in sleep and be enhanced by tapping. Although our patient has yet to have a seizure, these discharges likely represent a pathologic interictal electrographic correlate to his epileptic encephalopathy since the location and morphology are the same as his ESES discharges.
Further Reading:
- de Marco P, Tassinari CA. Extreme somatosensory evoked potential (ESEP): an EEG sign forecasting the possible occurrence of seizures in children. Epilepsia. 1981 Oct;22(5):569-75. PubMed PMID: 6793354.
- de Marco P, Calzolari S. Tactile evoked spikes in children. Epileptic Disord. 1999 Jun;1(2):113-9. PubMed PMID: 10937141.
- Langill L, Wong PK. Tactile-evoked rolandic discharges: a benign finding?. Epilepsia. 2003 Feb;44(2):221-7.PubMed PMID: 12558578.
