
- About ACNS
- Meetings
- Education
- Practice
- Research
- Advocacy
- Membership
Featured Case
Contributed by Robyn Whitney, MD
The Hospital for Sick Children; Toronto, Canada
A 15 month-old boy presented with new onset paroxymsal events over the preceding two weeks. The events consisted of repeated abduction of the right arm which was sometimes accompanied by a slight jerk, occuring in clusters lasting three to five minutes. The events occurred primarily in the evening and during periods of drowsiness. At maximum, they were occuring twice per night.
At age 3 weeks of age, the boy had been diagnosed with cerebral sinus venous thrombosis (CSVT), which resulted in a hemorrhagic infarction involving the left thalamus and left frontal parietal white matter. He did not have any acute seizures at that time.
Physical examination revealed a left hand preference, slightly increased tone in the distal right lower extremity and slightly brisker reflexes in the right upper and lower extremities compared to the left. A routine scalp EEG demonstrated the findings illustrated in Figures 1 and 2.
Questions: What does this EEG pattern represent? What is the diagnosis?
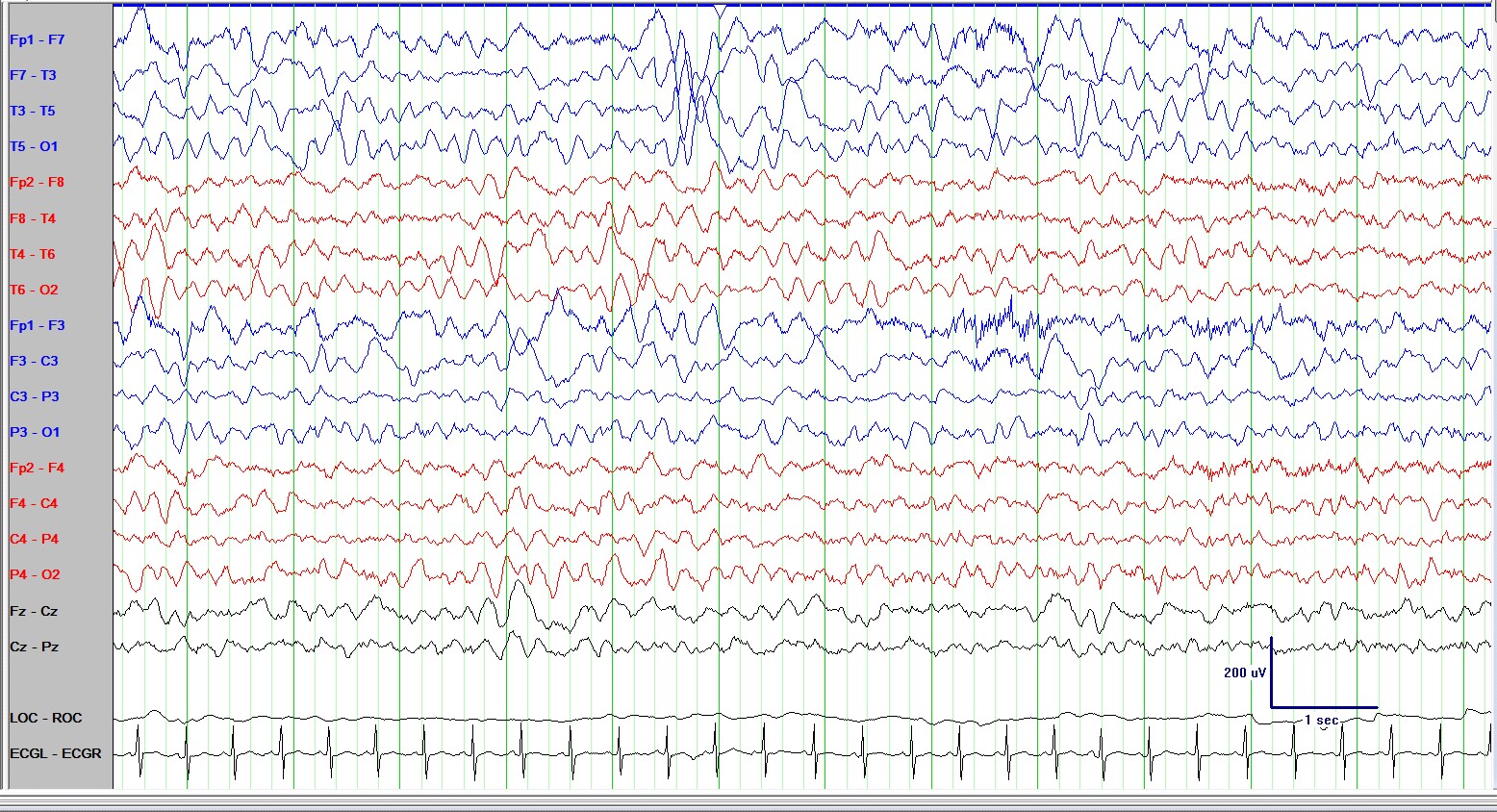
Figure 1. Routine EEG in wakefulness on an AP bipolar montage displayed at 10μV/mm, LFF= 1Hz, HFF=70 Hz, timebase = 30 mm/sec. Pz’ was used as reference. Intermittent left frontal and temporal sharp waves and spikes are seen, accompanied by continuous focal slowing.

Figure 2. Routine EEG in NREM sleep. AP bipolar montage displayed at 10μV/mm, LFF= 1Hz, HFF=70 Hz, timebase = 30 mm/sec. Pz’ was used as reference. During sleep, the left hemispheric background activity consists of high-amplitude delta activity with admixed high-amplitude multifocal spikes seen maximally over the left frontal and temporal head regions, but at times also over the left central and parietal head regions. Sleep spindles are seen in the right central head region, but not the the left central head region.
Answer & Discussion:
The EEG demonstrates hemi-hypsarrhythmia and the clinical history is consistent with asymmetric infantile spasms involving the right upper extremity. West syndrome is characterized by the triad of infantile spasms, hypsarrhythmia and developmental delay. The usual age of onset is between 4-12 months of age with a peak at 6 months of age. The classic EEG finding is hypsarrhythmia, characterized by very high-voltage, disorganized, chaotic and asynchronous slow waves (usually > 300μV), with superimposed multifocal spikes or sharp waves. Periods of generalized electrodecrement are seen throughout the recording and may be associated with clinical spasms. Hypsarrhythmia is often more pronounced during NREM sleep. In fact, the background activity during wakefulness may even be normal. Therefore, when evaluating a child for suspected infantile spasms the EEG recording should always include a period of sleep.
Several variations or modifications of the classic hypsarrhythmia pattern were described by Hrachovy and colleagues in 1984: 1) hypsarrhythmia with increased interhemispheric synchronization; 2)asymmetric hypsarrhythmia; 3) hypsarrhythmia with a consistent focus of abnormal discharges; 4)hypsarrhythmia with episodes of voltage attenuation (burst-suppression variant); and 5) hypsarrhythmia with little spike or sharp wave activity. Asymmetric hypsarrhythmia or hemi-hypsarrhythmia is characterized by the presence of hypsarrhythmia with a consistent amplitude difference between both hemispheres. Interestingly, it has been noted that the hypsarrhythmic activity may be maximally expressed over either the anatomically more abnormal hemisphere or the more normal hemisphere. Hemi-hypsarrhythmia is almost always associated with an underlying structural abnormality such as a cortical malformation (i.e. hemimegalencephaly) or a stroke, and should therefore prompt a neuroimaging evaluation. In our case, the hemi-hypsarrhythmia correlated with the previously-acquired left-hemispheric stroke.
Treatment of infantile spasms is aimed at both eliminating the clinical spasms and normalizing the EEG, or at least abolishing the hypsarrhythmia pattern. Standard medical therapy includes the use of vigabatrin, prednisolone or ACTH. The ketogenic diet may also be successful. In children who fail to respond to medical or diet therapy, resective epilepsy surgery should be considered, particularly when a structural brain lesion can be identified.
Further Reading: