
- About ACNS
- Meetings
- Education
- Practice
- Research
- Advocacy
- Membership
Contributed by:
James D. Triplett B.Med and Ruple S. Laughlin, MD
Mayo Clinic Rochester
A 79 year-old male with history of chronic lymphocytic leukemia (CLL) on irbutinib for 10 months presented for neuromuscular evaluation due to an 8 month history of fatigue, lower extremity weakness and occasional calf cramping. Further history revealed development of postural dizziness, >15 Lb weight loss and constipation over the last 6 months. Examination demonstrated mild weakness of left ankle inversion and iliopsoas bilaterally. Sensory examination showed absent vibration sense at the toes and without deep tendon reflex abnormalities. Serological evaluations revealed a normal creatinine kinase of 40 (U/L) and low level N-type voltage gated calcium channel antibodies (0.09 nmol/L). Electrodiagnostic testing was recommended to further evaluate his symptoms.
Nerve conduction studies revealed normal amplitude compound muscle action potentials with reduced motor conduction velocities in the left upper and lower extremities. F-wave latencies were not prolonged compared to F-wave estimate. The median sensory nerve action potential (SNAP) was attenuated with prolonged distal sensory latency. The sural and ulnar SNAPs were normal but the R1 blink latency was mildly prolonged. 2 hertz repetitive stimulation of the left fibular and ulnar nerves demonstrated neither decrement nor facilitation after brief exercise.
Needle electromyography (EMG) examination revealed early recruitment of mixed long and short duration polyphasic motor unit potentials with occasional fibrillation potentials in distal lower extremity muscles. Proximal upper and lower limb muscles revealed small, polyphasic, rapidly recruited motor unit potentials, not accompanied by fibrillation potentials or myotonic discharges. Overall, needle EMG findings were most concerning for an underlying myopathy with the NCS findings suggesting some degree of overlying motor predominant neuropathy with predominantly demyelinating features as well as a left median neuropathy at the wrist.
Electrodiagnostic findings supported proceeding with muscle biopsy, which was performed of the right gluteus medius. Pathology was consistent with systemic amyloidosis-associated myopathy. Amyloid subtyping showed this to be ATTR (transthyretin)-type amyloid deposition.
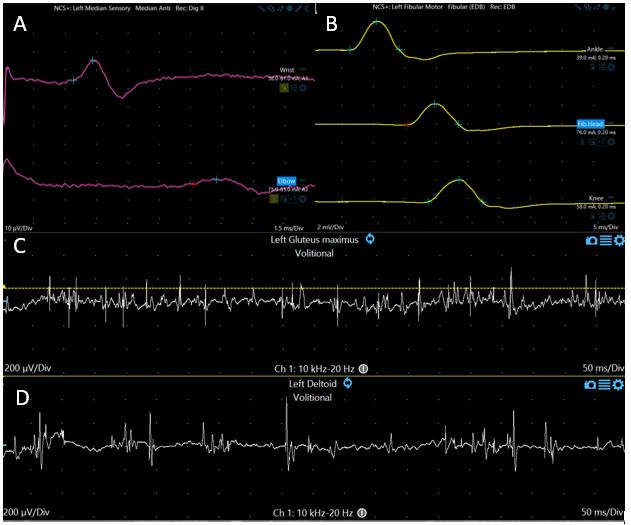
Figure 1: (A) Left median sensory nerve conduction study: distal sensory latency 4.3 msec (normal <3.6 msec), amplitude 11 mV (normal >15) mV, sensory conduction velocity 47 m/sec (Normal >56 m/sec) (10µV/Div, 1.5msec/Div); (B) Left fibular motor nerve conduction study: distal motor latency 6.3 (normal <6.6), amplitude 2.3 mV ( normal >2 mV) conduction velocity 30 m/sec (normal >41 msec) (2mV/Div, 5msec/Div); (C)EMG left gluteus maximus revealing low amplitude, short duration motor unit potentials (200µV/Div, 50msec/Div); (D) EMG of left deltoid revealing low amplitude, short duration polyphasic motor unit potentials (200µV/Div, 50msec/Div)
Question 1: Is CK typically elevated in systemic amyloidosis-associated myopathy?:
Question 2: The presence of median neuropathy at the wrist is rarely encountered in systemic amyloidosis:
Question 3: The concentric needle examination finings in amyloid myopathy are similar to other chronic inflammatory myopathies?