
- About ACNS
- Meetings
- Education
- Practice
- Research
- Advocacy
- Membership
Contributed by
Esther Bui MD, FRCPC; Danielle Andrade MD, MSc; and Richard Wennberg MD, PhD, FRCPC
Toronto Western Hospital; Toronto, Canada
A 23-year-old woman, previously well, presented with headache and sore throat. She was prescribed antibiotics for sinusitis. Five days later, she presented to the emergency department with manic symptoms and psychosis. Antipsychotics were prescribed and she was hospitalized. One week later, she became febrile with a temperature of 38.6 degrees Celsius. On examination, she was confused, diffusely rigid with a generalized tremor and dystonia involving the face, tongue and mouth. She subsequently had a generalized tonic-clonic seizure requiring intubation. MRI brain was normal. Cerebrospinal fluid analysis identified lymphocytic pleocytosis. Infectious disease work-up was negative. An EEG performed in the intensive care unit demonstrated the findings illustrated below.
What is this EEG finding and what is the most likely diagnosis?
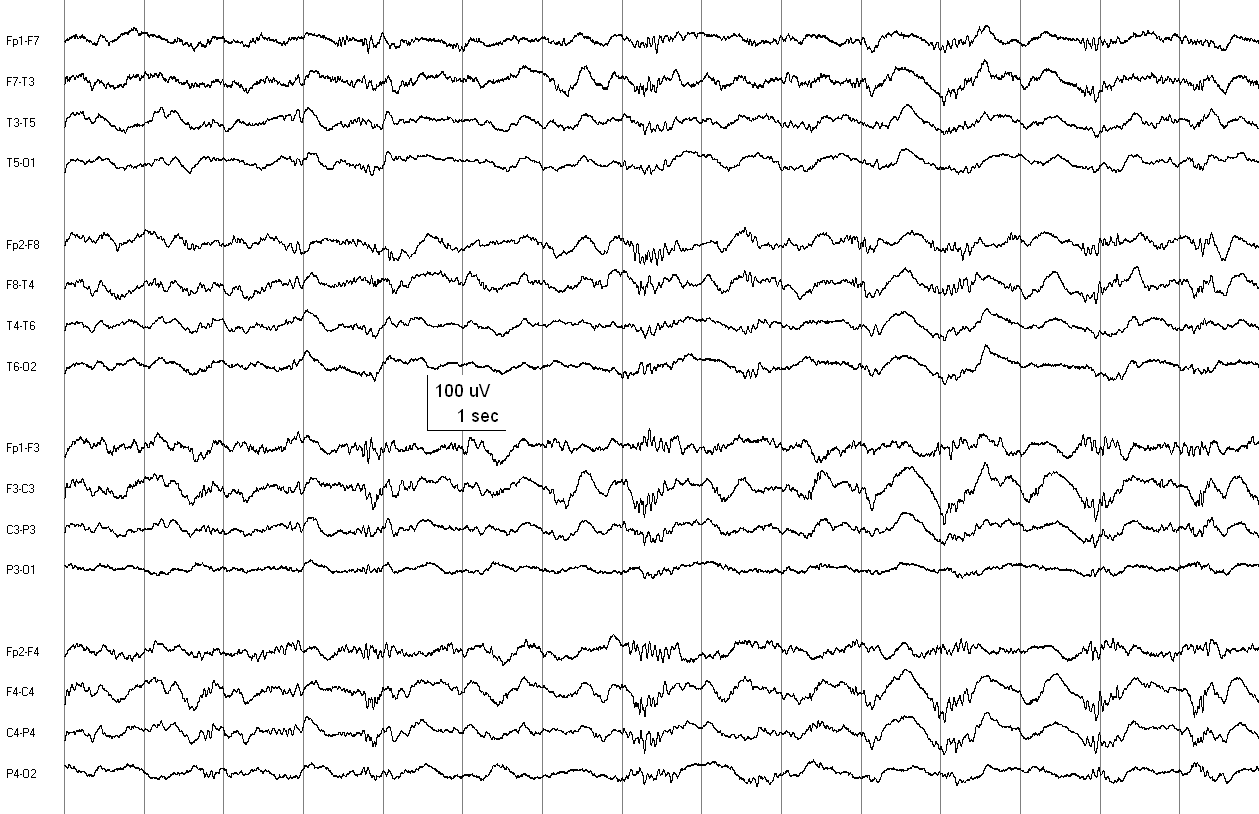
Figure: Routine EEG in an A-P longitudinal bipolar montage. TC = 0.3 sec; HFF = 70 Hz.
Click HERE to visit the ACNS website for the Answer and Discussion!
Anti-NMDA receptor encephalitis is an autoimmune encephalitis first identified in 2007 which is characterized by neuropsychiatric symptoms, seizures, movement disorders, dysautonomia, hypoventilation and coma (1, 2). The condition has been associated with ovarian teratoma in young women, testicular teratoma in men and small cell lung cancer (2, 3). However, nearly half of described cases have no identified tumor.
Historically, EEG has had limited utility in the diagnosis of autoimmune encephalitis because only non-specific EEG patterns were described, such as continuous slow waves and frontal intermittent rhythmic delta activity (FIRDA)(4). However, in 2012 a novel EEG feature, extreme delta brushes (EDB), was reported to be associated with anti-NMDA receptor encephalitis. This EEG pattern was named due to its morphological similarities with delta brushes, a neonatal EEG feature of prematurity (5). EDB consist of generalized rhythmic delta wave activity with overriding bursts of 20-30 Hz beta activity. In two separate case series, EDB were identified in approximately one third of anti-NMDA receptor encephalitis and in one case series they were associated with status epilepticus (5, 6). To our knowledge, EDB have not been identified in other forms of encephalitis. Although the significance of EDB remains uncertain, some authors have observed an associated poorer prognosis (5) whereas others, while not observing this, did associate this pattern with cases requiring more aggressive and intensive medical management (6).
In our patient the diagnosis of anti-NMDA receptor encephalitis was confirmed by the identification of anti-NMDA receptor IgG antibodies in cerebrospinal fluid by immunofluorescence assay. The patient subsequently underwent tumor surveillance including MRI and ultrasound of the pelvis and whole body PET scan, all of which were negative. Despite aggressive immunosuppressant therapy including steroids, plasmapheresis and intravenous immunoglobulin, the patient’s clinical status continued to deteriorate. Therefore, the decision was made to proceed with bilateral oophorectomy in order to remove a possible occult ovarian teratoma, and a 2.5 cm mature cystic teratoma was indeed identified on pathology of the right ovary.
EDB is a novel EEG feature that when recognized in patients with new onset encephalitis may further help confirm the diagnosis of anti-NMDA receptor encephalitis and guide potential treatments and outcomes for patients. However, the precise sensitivity and specificity of EDB for anti-NMDA receptor encephalitis remain to be determined.
References:
(1) Taylor RB, Mason W, Kong K, Wennberg R. Reversible paraneoplastic encephalomyelitis associated with a benign ovarian teratoma. Can J Neurol Sci. 1999 Nov;26:317-20.
(2) Dalmau J, Tüzün E, Wu HY, Masjuan J, Rossi JE, Voloschin A, Baehring JM, Shimazaki H, Koide R, King D, Mason W, Sansing LH, Dichter MA, Rosenfeld MR, Lynch DR. Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol. 2007 Jan;61:25-36.
(3) Dalmau J, Gleichman AJ, Hughes EG, Rossi JE, Peng X, Lai M, Dessain SK, Rosenfeld MR, Balice-Gordon R, and Lynch DR. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol. 2008 Dec;7:1091-8.
(4) Baysal-Kirac L, Tuzun E, Altindag E, Ekizoglu E, Kinay D, Bilgic B, Tekturk P, Baykan B. Are There Any Specific EEG Findings in Autoimmune Epilepsies? Clin EEG Neurosci. 2015 Aug 2 [Epub ahead of print].
(5) Schmitt SE, Pargeon K, Frechette ES, Hirsch LJ, Dalmau J, Friedman D. Extreme delta brush: a unique EEG pattern in adults with anti-NMDA receptor encephalitis. Neurology. 2012 Sep;79:1094-100.
(6) Veciana M, Becerra JL, Fossas P, Muriana D, Sansa G, Santamarina E, Gaig C, Carreño M, Molins A, Escofet C, Ley M, Vivanco R, Pedro J, Miró J, Falip M; In behalf of the Epilepsy Group of the SCN. EEG extreme delta brush: An ictal pattern in patients with anti-NMDA receptor encephalitis. Epilepsy Behav. 2015 Aug;49:280-5.